Entry
The Imperative of Smarter Clinical Information Systems
How AI agents and openEHR can lift healthcare out of its purgatory by structuring every input and embedding it into durable clinical knowledge.
Filed9 min readvia substack
00 / Masthead
Entry
How AI agents and openEHR can lift healthcare out of its purgatory by structuring every input and embedding it into durable clinical knowledge.
How AI agents and openEHR Can Lift Healthcare Out of Its Purgatory
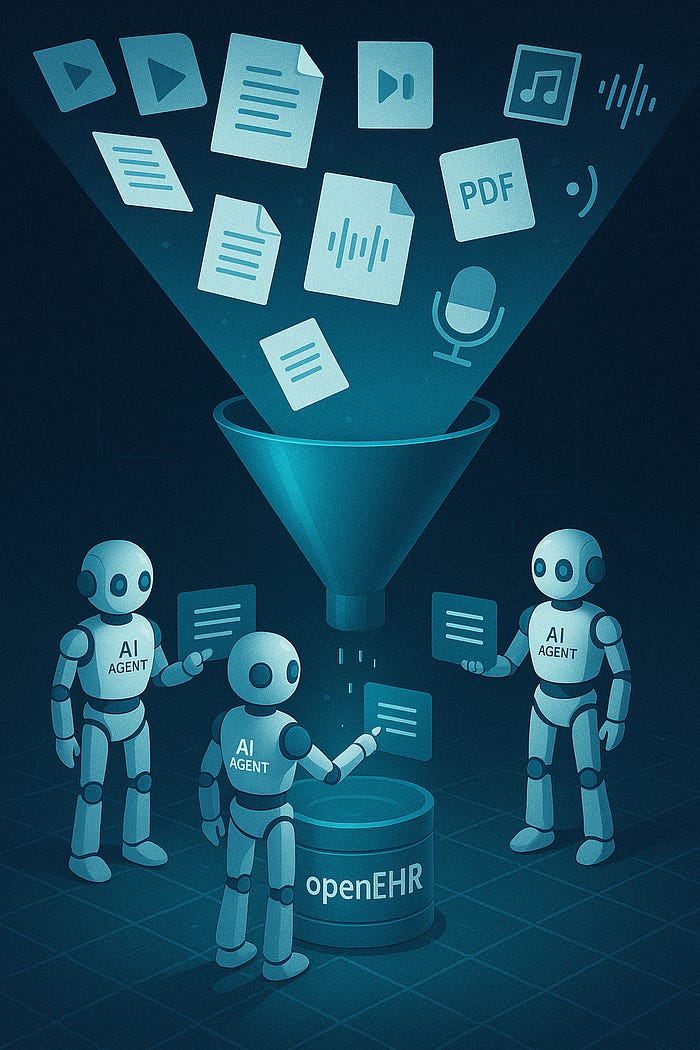
TL;DR - Hospitals don’t need more bolt‑on AI dashboards; they need to stop spending human hours transcribing voice notes, scanned referrals, and faxes into databases. Multimodal AI can now structure any input, and openEHR turns that structure into lasting, shareable knowledge. The combo wipes out form fatigue, bridges wildly different local workflows, and fades into the background so clinicians can get back to medicine.
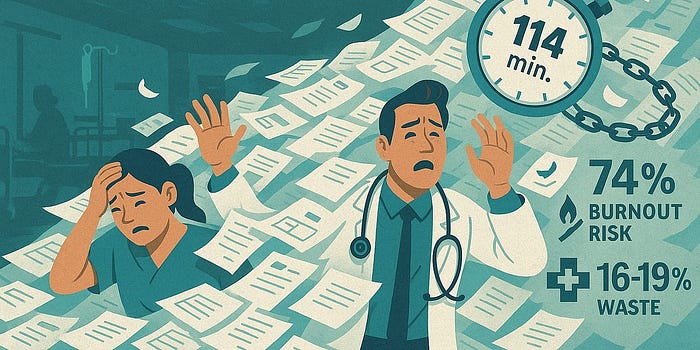
Across the globe, healthcare is wrestling with more than flashy new tech - it’s staring down an economic crunch that hits clinicians right where it hurts: time. Administrative chores siphon off billions, drive burn out to record highs, and threaten the financial breathability of hospitals.
I watch it daily. As Lead of AI Engineering at Cistec AG - makers of KISIM, Switzerland’s leading CIS (Clinical Information System) - we see flashy pilots developed elsewhere stall because they bolt beside existing workflows instead of inside them: another login, another window, more juggling for doctors and nurses already juggling too many.
It’s time for a CIS revolution. Fuse mature, multimodal, agentic AI with openEHR’s clinician‑curated data models and the intelligence disappears into the flow. Notes dictate themselves, documents self‑organize, forms pre‑fill - backed by structured, clinically validated data you can trust.
Crack the admin problem first and you unlock capacity, morale, and cash for everything else.
Swiss healthcare’s admin bill isn’t just a line item; it’s ballast. The numbers and ward‑floor stories say it all:
Hospitals pay in cash, too: a federal audit pegs 16–19 % of spending as avoidable waste - mostly duplicated data entry and information chasing.
🌍 And this isn’t just Switzerland. The same documentation purgatory spans every corner that practices modern medicine.
Absurd 2025 scene: junior doctors act as digital scribes, copy‑pasting diagnoses and medication lists from old PDFs or referrals, then re‑prescribing every drug one field at a time. Clinical value added: zero. Human frustration: max.
Why “Fix It Later” Is No Longer an Option
Every day we stall, that paperwork drag converts directly into overtime invoices, locum fees, and missed‑revenue leaks. Solving it isn’t about shaving ten seconds off a dialog box; it’s about rewiring how data is captured and reused.
When all information is structured once and reused everywhere, four levers move together:
1. 🩺 Free Capacity, Cut Burnout
Automation lifts the slog of dictations, PDFs, and faxes, handing back hours for patient care and trimming locum spend.
2. 💼 Super‑charge Operational Intelligence
openEHR‑clean data turns bed, theatre, and staffing planning into data science, not educated guesswork.
3. 🔧 Build Longitudinal Gold
Notes, vitals, and labs stack into lifelong patient timelines - fuel for today’s quality metrics and tomorrow’s precision medicine.
4. 💸 Slash Error Loops & Hidden Costs
Capture data right the first time and you eliminate claim denials, audit rework, and those “please re‑send” calls all while averting safety events born of missing info.
Pan‑European studies peg the upside in the multi‑billion‑franc range, and Switzerland’s own 2023 digital‑transformation program calls for exactly this structure‑first playbook.
Bottom line: the human toll makes action urgent; the economic math makes delay indefensible. Time to break the paperwork ballast and let hospitals breathe.
So, how do we build a CIS that actually reduces friction and disappears into the workflow? It takes two core components working in tight synchrony: the rock-solid, clinically validated data structures of openEHR, and the flexible, context-aware processing power of multimodal AI agents. Forget bolt-on dashboards; this is about embedding intelligence from the ground up.
If AI is the muscle, openEHR is the skeleton that keeps it aligned and safe. Hospitals aren’t adopting this open standard for fun; they’re choosing it because nothing else reliably converts messy clinical reality into computable, shareable, future-proof knowledge while keeping clinicians in control. Here’s the crucial difference it makes:
Bottom line: openEHR provides the essential trust layer. It ensures that the “invisible” AI operates within safe, clinically agreed-upon boundaries.
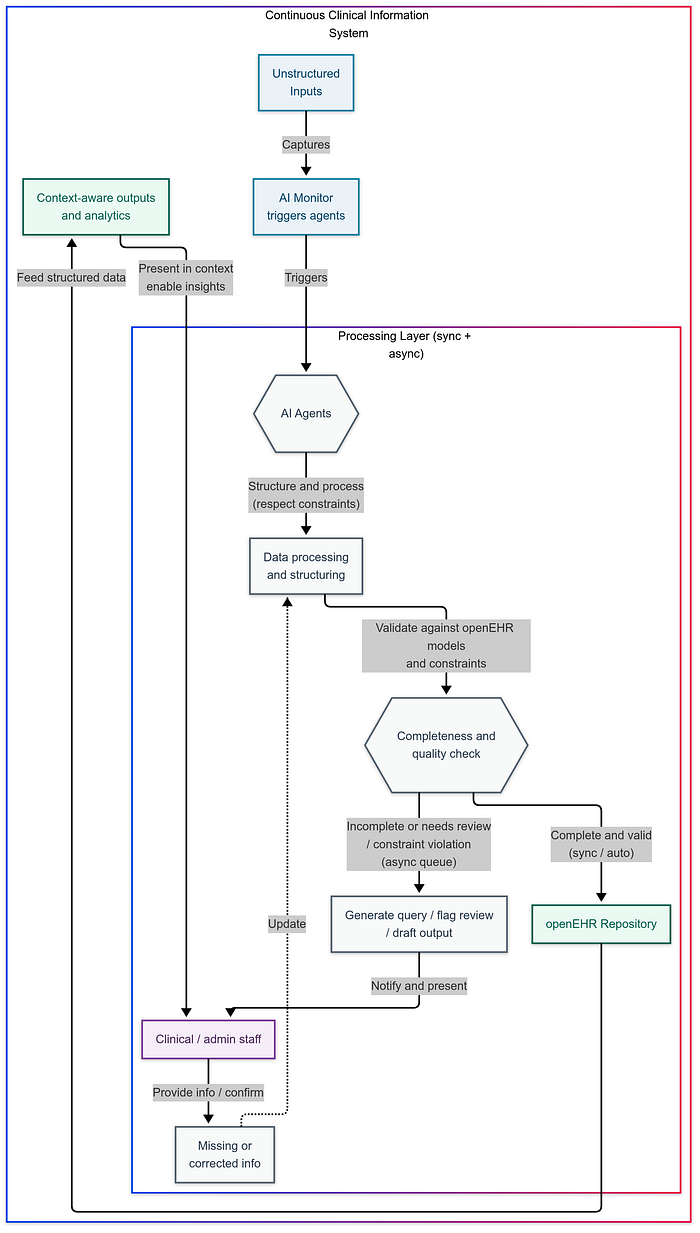
Unstructured inputs hit AI agents that auto‑structure and validate against openEHR rules. Good data is stored instantly; anything incomplete lands in an async queue for quick clinician review. Once inside the repository, it powers context‑aware outputs: no extra dashboards required.
If openEHR defines the trustworthy “what” of the data, AI agents handle the “how” - processing information and automating tasks with minimal friction. They understand context, handle diverse inputs, and interact naturally, always respecting the openEHR guardrails:
Tuesday 07:03 - Dictation captured ambiently, key vitals automatically extracted and validated, AI flags a potential medication interaction for human review based on the structured record, initiates a query for a rehab bed based on documented goals, and drafts the handover note incorporating all validated data. Zero extra clicks, zero context switches.
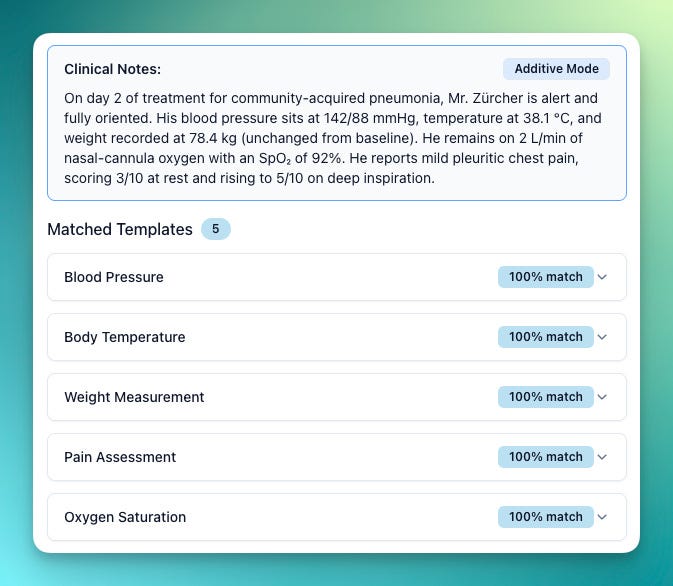
Our prototype agent maps a live voice note to standard openEHR concepts: confidence scores determine what’s automatically structured (100 %) vs. what still needs a human glance. In production this would happen transparently behind the scenes.
Once your information sits as clean, trustworthy openEHR records, admin efficiency is just the opening act. That foundation unlocks a stack of high‑value moves with almost no extra lift:
💸 **Super‑charged coding & billing **Agents mine the structured narrative, surface / CHOP / TARMED codes, and flag the quirky edge cases for a two‑second human sweep - slashing manual effort and boosting revenue integrity.
🏥 **Clinically‑aware resource insights **With patient acuity, diagnoses, and interventions all computable, the AI can forecast bed demand, spot discharge bottlenecks, and optimize patient flow based on real clinical drivers - not gut feel.
🛡️ **Streamlined authorizations & compliance **Need prior approval? The agent bundles the exact clinical rationale straight from the record, checks it against quality measures, and flags gaps before auditors - or insurers - do.
📊 **Effortless reporting **Quality metrics, admin KPIs, registry feeds, all generated automatically from the validated data store. Accurate, consistent, and on time, minus the spreadsheet heroics.
🔬 **Powerful cross‑patient insights **Want every patient with a tricky comorbidity pattern? Or outcomes across a demographic slice? Longitudinal, structured data makes complex queries routine, driving better care pathways and sharper population‑health research.
Structure the data once, and the payoff keeps compounding.
Technology is only half the battle; success hinges on thoughtful rollout and human factors:
Building trust in this ‘invisible’ layer is paramount. That requires clear guardrails:
Let’s be clear: this isn’t vaporware. My team and I at CISTEC are already actively researching and building this vision today at the same time as introducing immediate high-impact AI features on top of our existing platform.
This is however, still a journey and not a finished product. I’ll be sharing the real story - progress, hurdles, and demos - at the 2nd openEHR.ch Symposium on May 5th, 2025. Hope to see you there.
Alright, let’s land this plane. The takeaway? Healthcare isn’t just inefficient; it’s actively hostile to clinicians’ time and focus thanks to clunky systems and that soul-crushing “ workflow tax.” Just creating poorly integrated AI dashboards isn’t the answer.
The real fix starts deeper: using AI agents to intelligently structure every piece of information - voice notes, scanned docs, sensor streams - and locking it down reliably with openEHR’s clinician-defined rules. That combo gives you data you can trust and intelligence that works for you, one that disappears into the workflow.
The system I’ve outlined here slashes avoidable costs, turbo‑charges decision‑making, and lifts care quality - all while handing clinicians the gift of time. The tech is ready, the ROI is on the table, and the need is impossible to ignore. Let’s replace today’s documentation sinkhole with systems that let doctors and nurses spend their time on medicine - not paperwork.
Originally published at https://bytesizedbrainwaves.substack.com.